Hayward, Peters, van Bockxmeer, Seow, McKitrick, and Canyon explore the efficacy of public health communication on community decision-making during an air pollution crisis in Perth.
A hazardous event involving a chemical fire results in the release of toxicants into community in the path of the smoke plume. Health outcomes can manifest in acute and chronic cancers, congenital abnormalities and psychosomatic distress. During a toxic crisis, accurate information needs to be distributed quickly and effectively. Once informed, individuals decide on a course of action, such as whether to evacuate or remain sheltered-in-place, that may critically impact their health and safety. Communication can be the most critical factor that determines the success of an emergency public health response (Bernhardt, 2004). Agencies in charge of managing crises need to efficiently and effectively communicate risks and instructions. Likewise, a trusting and accepting community is more likely to be compliant with instructions. Thus, even before the instructions are delivered, an individual’s opinion of the reliability of the communicating authority will affect compliance. Generally, trust in government, police, fire and emergency services, and information providers has diminished since the 1960s (Ludwig, 2007) and the public tends to be sceptical of visual information presented by the media (Orren, 1997). If organisations are perceived as trustworthy by the public, their use as information sources would be advantageous. The level of trust held in an organisation is influenced by including personality, experiences and economic status (Deurenberg-Yap et al., 2005). When comparing different institutions, public confidence of the medical community is generally considered to be higher than that of many others (Kiousis, 2001). In a crisis or high-risk situation, communities can have a higher level of trust in both government and medical organisations (Kasperson et al., 1992), and the public develops a broader societal trust (Koller, 1988).
During a crisis, the public tend to base decisions on perceived risk rather than on actual risk (Fischhoff et al., 2002). The knowledge that behaviour of an individual is directly related to personal risk perception (Slovic, 2000) has a bearing on how information can be effectively conveyed to people in a hyper-alert mental state. However, while much research has investigated the use and development of emergency response plans and the roles of leadership and communication in the event of a health crisis, there is a lack of evidence relating to the behavioural responses of a population in the event of crises. This study thus investigated the public’s level of trust in specific organisations and how the affected community formulate their decision to ignore or follow important health information.
The event selected for analysis was a scrap metal yard fire in the suburb of Bassendean, Western Australia which burnt for over two days (6-7th Dec 2004). The fire produced smoke and toxins from whitegoods (FESA, 2005) which formed a thick plume that spanned a number of northern and western suburbs within the city. While toxin concentrations were not high enough to produce health impacts (DoE, 2005, FESA, 2006b), measurable outcomes from the incident included loss of a 5000 m2 property, a damage bill of $3,000,000 and the involvement of more than 200 fire fighters (FESA, 2006a). Contaminated water run-off entered local drain tributaries to the major city river (PRU, 2005). Due to the scale of the incident, a multi-agency response was required including the Environmental Protection Agency’s Pollution Response Unit (PRU), the Fire Emergency and Services Authority (FESA), the Hazmat Emergency Advisory Team (HEAT), Department of Health (DoH), Department of Environment (DoE) and the WA Police. Management for this crisis was conducted under the guidelines of Westplan – Hazmat, the Western Australian Fire Emergency Management Plan (DoH 2004).
Directive information was provided to the public via the police, the Departments of Health and Environmental Protection, and general medical practitioners, who were provided advice by the Department of Health (PRU, 2005). Members of the public within range of the smoke plume were informed via media sources (TV, radio, print), a mobile repetitive loudspeaker announcement within 1.5 km of the fire whilst the plume was intact, and a public information evening involving all agencies was held two weeks after the event. When making the decision to recommend shelter-in-place or evacuation, decision makers need to evaluate factors that characterize the release, meteorological conditions, and populations that may be affected (Sorenson et al., 2004). In this case, the public were informed that there was minimal risk, but were directed to close air conditioning vents, to shelter-in-place, and to seek medical advice if experiencing adverse health effects (DoE 2005, PRU 2005, FESA 2006b).
The exposed population was geographically determined by the position of the plumage of the fire. Candidates were excluded if they were not in the exposure zone and if they could not recall the event or if they were under 18 yo. Door-to-door surveys were conducted by three interviewing teams and continued until a sample size of 101 participants had been acquired. An 18 question survey acquired demographic data (age, gender, marital status, highest education level and family status), and sought information on: a) behaviours of residents during the fire, b) compliance with information provided, c) most effective means of information transmission, and d) level of trust in information sources.
Bivariate statistical analysis involving Chi-Square tests employed SPSS v16. Differences were considered significant at p<0.05. This study was ethically cleared by the Human Research Ethics Committee, University of Western Australia (RA/4/1/1830).
Of the 983 houses visited, 535 were non-contactable and 347 did not participate because they were either new residents (n=128), could not recall the event (n=94), were unwilling to participate (n=121), or could not speak English (n=4). The participation rate was 22.54% and 101 surveys were completed with a gender ratio of ♂46.5:♀53.5%. Sixty-one percent of respondents completed a technical/trade certificate or university degree while 40% achieved primary school to high school completion.
Ninety-five participants received some information on the fire. Of these, 90 received information from the media, 33 from friends, 13 from the police, 2 from local government, 1 from a medical doctor and 1 from FESA. No information was recalled as being received from PRU. The fire caused considerable concern in the community with 35.6% of the population believing the incident posed an immediate risk. When participants were asked to recall the nature of the advice provided through all communication channels, 15% could not remember, 31% said shelter-in-place, 54% said shelter according to FESA specifications, one said go look at the fire and none said evacuate. While age and education were not significant, there were significant gender differences in the recall of shelter-in-place (♂21:♀10) and shelter with FESA actions (♂18:♀36).
When participants were asked how they were informed, results indicated that loudspeaker, media and phone/SMS were recalled the most although several other methods were used (Fig 1). Significantly more males recollected the use of loudspeakers (20 vs. 13%), while significantly more women recalled receiving information via phone/SMS (19 vs. 4%). Significantly more participants aged over 40 recalled loudspeakers (31 vs. 2%) and phone/SMS (14 vs. 9%). Media was equally remembered by all participants and level of education was not significant.
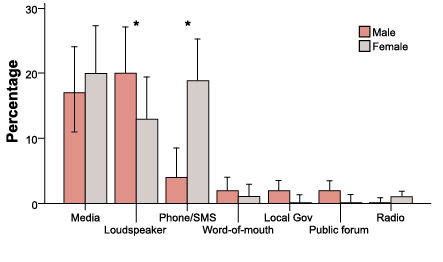
1a. Gender
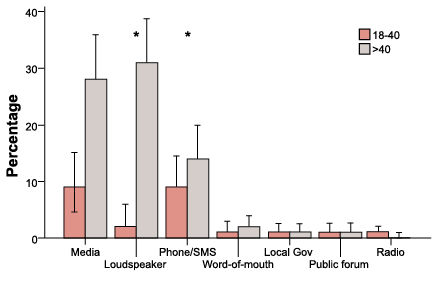
1b. Age
Figure 1. Communication channels that were recalled by the exposed public by gender (a) and age (b). Error bars 95% CI. Significant differences between gender and age groups are indicated by an asterisk - Pearson Chi-Square p<0.05.
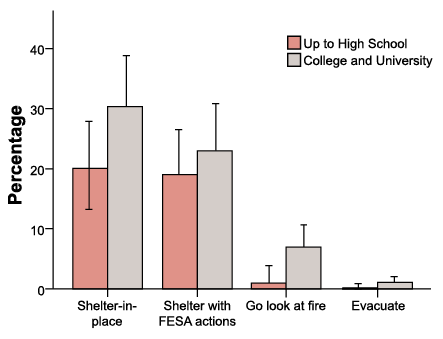
Following this advice, 49.5% of participants sheltered-in-place, 42.6% sheltered according to FESA specifications, 7.9% went to see the fire and 0.9% evacuated. Gender, age and education were not significant (Fig. 2). Seven percent of higher educated participants and only 1% of lesser educated participants went to see the fire.
2a. Gender
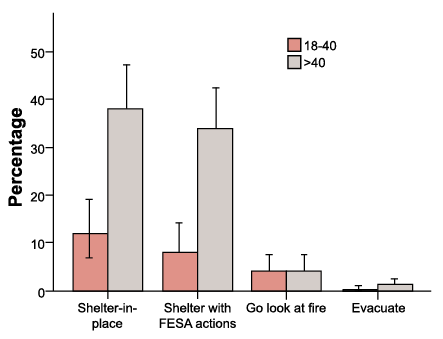
2b. Age
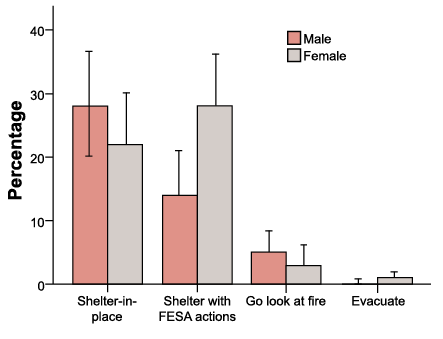
2c. Education
Figure 2. Decisions made by the public in response to communications from various sources about a toxic plume from a chemical fire by gender (a), age (b) and education (c). Error bars 95% CI – no significant differences observed.
Participants based their decisions on intuition (41%), media sources (31%), multiple sources (14%), family (8%), police (5%) and doctors (1%). While no significant differences emerged due to gender, age and education, there were some interesting observations (Fig. 3 abc). Men were more inclined to base their decisions on intuition than women (55 vs. 45%), and women were more inclined to base their decisions on information received from multiple sources than men (71 vs. 29%). Older participants were more likely than younger participants to rely on intuition (71 vs. 29%) and more educated participants were twice as likely to rely on intuition (67 vs 33%) and media sources (65 vs. 35%) than younger and less educated participants.
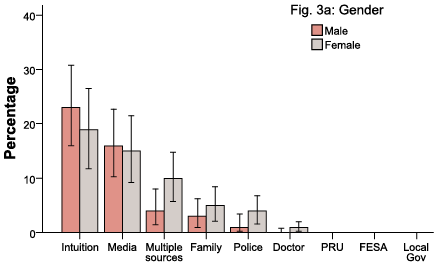
3a. Gender
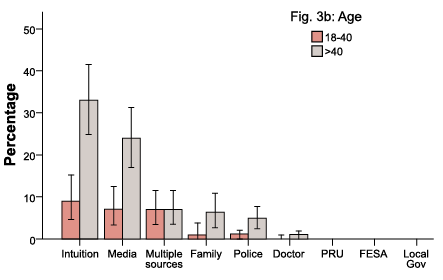
3b. Age
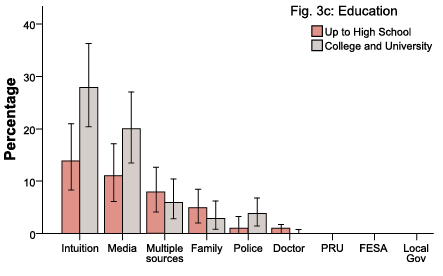
3c. Education
Figure 3. Responses by gender, age and education to the question, “Which source of information did you base your decision on?” Error bars 95% CI – no significant differences observed.
Trust in information sources was ranked from one to seven, with seven indicating high trust (Fig. 4).
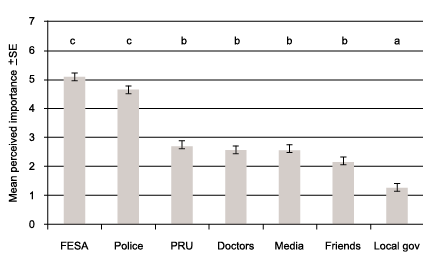
Figure 4. Seven information providers that would be most trusted in a similar crisis event. Higher scores on the Y axis indicate increasing importance while alphabetical characters indicate significant differences (p<0.05).
Twenty-five percent of participants stated that they would act differently in the future: 8% of participants said they would evacuate, 7% said they would seek out additional information, 6% said they would do a better job of sheltering and 2% said they would do a better job of avoiding the smoke due to pre-existing asthma.
This study resulted in several important findings relating to perception of risk, type of communication authorities, method of communication, nature of advice, decision in response to advice, most trusted advice provider, and likelihood of behavioural change. Recall was fairly high with 32% remembering the basics and 54% remembering specifics. Advice recall was fairly good with only 15% unable to remember details. Inability to recall was not significantly related to age.
A third of the population perceived the fire to pose a threat which was in direct contrast to suggestions that the exposed population was highly concerned about the immediate risks posed by the air pollution crisis (PRU, 2005). Alternative explanations for the high compliance rate are: a) the information distributed during the crisis was sufficient to enable correct acute decision making to occur, b) the population had some prior knowledge on how to act during an acute air pollution incident, c) sheltering in place is the compliant, normal reaction. Burgess et al. (2001) suggested that personal perception of risk is a key element since low evacuation rates are associated with chemical release events involving substances with relatively lower vapour pressures and hazard indices in open-air locations. Personal perception also played a strong role in influencing the decision to go see the fire. That all but one of the 8%, who approached the fire after receiving advice to the contrary, were well educated either points to greater curiosity imparted by their training or greater apathy (Zavestoski et al, 2004) towards environmental contamination.
Decisions to act during an acute air pollution crisis are influenced by gender with a higher percentage of males choosing to act on their own intuition rather than on the information provided. Reliance on intuition indicates that despite extensive efforts to communicate using the police and media, much of the population will still base their decisions on their own instincts, past experiences and prior knowledge. After personal intuition, a third of the population based their decisions on information received from the media. This might be accounted for by high exposure to media within the population in contrast to other information sources. Other researchers have found that younger participants are more likely to contact multiple sources (Muha, 1998), but this was not supported here.
During exposure crises, information should be transmitted through trusted organisations, these being the police, fire and emergency services. It is important for the same organisations to be involved in information delivery during every crisis event because public perception of the authenticity of information provided to them by an organisation influences their trust in that organisation in the future (Lang, 1998). It is also important to train the public. That 8% more people would change their behaviour to evacuate during a similar event indicates that information is lacking in some areas or is not fully understood. Increased awareness campaigns may thus reduce unnecessary evacuations and their associated risks and resource implications (Kinra et al., 2005). The most effective communication to the public will depend on the age mix of the population and will change over time. For the surveyed population, media, loudspeaker and phone/SMS were seen as being the most effective means of providing information. But, as the proportion of mobile phone users grows, SMS is likely to become an increasingly important means for the communication of emergency public health information. The agencies involved in providing information believed that their advice was transmitted effectively with efficacious outcomes. However some members of the public disputed these claims at the community forum held shortly following the fire (FESA, 2005, PRU, 2005).
The results from this study indicate that crisis communication should be tailored to take community characteristics into account so that unnecessary exposure to hazardous airborne pollutants is limited. Crisis communicators should be aware that tailoring will need to be adjusted over time as technologies become more available and accepted by the population. Improvements in crisis communications efforts in Perth are required to address the concerns of 55% of the population who felt incompletely informed.

Hazardous airbourne pollutants.
Bernhardt, J., 2004, Communication at the core of effective public health. American Journal of Public Health 94: 2051-2054.
Burgess, J. L., Kovalchick, D. F., Harter, L, Kyes, K. B., Lymp, J. F. and Brodkin, C. A. (2001) Hazardous materials events: evaluation of transport to health care facility and evacuation decisions. American Journal of Emergency Medicine 19: 99-105.
DoE. (2005) Fears of toxic cocktail sparks major pollution emergency response. Sustainability, Official Newsletter of the Department of Environment, Western Australia 6: 2.
DoH. (2004) Bassendean scrap metal yard smoke results reassuring. Department of Health. [cited April 2008] http://www.health.wa.gov.au/press/view_press.cfm?id=490.
Deurenberg-Yap, M., Foo, L. L., Low, Y. Y., Chan, S. P., Vijaya, K. and Lee, M. (2005) The Singaporean response to the SARS outbreak: knowledge sufficiency versus public trust. Health Promotion International 20: 320-326.
FESA. (2005) Annual Report 2004/2005, Fire and Emergency Services Authority of Western Australia, Perth.
FESA. (2006a) State emergency hazard plans. Fire and Emergency Services Authority of Western Australia, Perth.
FESA. (2006b) Hazardous materials. Fire and Emergency Services Authority of Western Australia, Perth.
Fischhoff, B., Bostrom, A., & Quadrel, M.J. (Detels, R., McEwen, J., Beaglehole, R. and Tanaka, H. eds.) (2002). Risk perception and communication: Oxford Textbook of Public Health pp. 1105-1123. Oxford University Press, London.
Kasperson, R. E., Golding, D. and Tuler, S. (1992) Social distrust as a factor in siting hazardous facilities and community risks. Journal of Social Issues 48: 161-87.
Kinra, S., Lewendon, G., Nelder, R., Herriott, N., Mohan, R., Hort, M., Harrison, S. and Murray, V. (2005) Evacuation decisions in a chemical air pollution incident: cross sectional survey. BMJ 330: 1471-1476.
Koller, M. (1988) Risk as a determinant of trust. Basic and Applied Social Psychology 9: 265-276.
Lang, T. (Ratzan, S. C. ed) (1998) BSE and CJD: recent developments: The Mad Cow Crisis: Health and the Public Good. UCL Press, London.
Ludwig, J. (2007) FOI reforms vital for public trust in government. Information Management Conference, Melbourne 22 Aug.
Muha, C. (1998) The use and selection of sources in information seeking: The cancer information service experience. Part 8. Journal of Health Communication 3: 109-120.
Orren, G. (Nye, J. S., Zelikow, P. D. and King, D. C. eds.) (1997) Fall from grace: the public’s loss of faith in government: Why Americans Mistrust Government. Harvard University Press, Massachusetts.
PRU. (2005) Smorgon incident report. Pollution Response Unit, Department of Environment, Perth.
Slovic, P. (2000) The perception of risk. Earthscan, London.
Sorenson, J. H., Shumpert, B. L. and Vogt, B. M. (2004) Planning for protective action decision making: evacuate or shelter-in-place. Journal of Hazardous Materials A109: 1–11.
Spence, P. R., Lachlan, K., Burke, J. M. and, Seeger, M. W. (2007) Media use and information needs of the disabled during a natural disaster. Journal of Health Care for the Poor and Underserved 18: 394-404.
Zavestoski, S., Agnello, K., Mignano, F. and Darroch, F. (2004) Issue framing and citizen apathy toward local environmental contamination. Sociological Forum 19: 255-283.
Anna Hayward, Kate Peters and John van Bockxmeer are 5th year medical students studying at University of Western Australia with Dr Canyon and Dr McKitrick as their supervisors. Dr Seow manages the Perth Pollution Response Unit and requested this study. Dr. Deon V. Canyon is from the School of Public Health, Tropical Medicine and Rehabilitation Sciences, James Cook University.
Dr. Canyon is the corresponding author for this paper and can be contacted on phone: +61-8-9385 9415 or via E-mail: deoncanyon@gmail.com

